61 yr old male with SOB and involuntary movements of both upper limbs
Note - This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centred online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment.
5 September 2022
M.G.Prasanna Lakshmi
Roll no 93 (2k18 batch)
Case -
A 61 y/o male, resident of Dubbaka, Ramanapet
came to the OPD with chief complaint of SOB since 10 days.
History of presenting illness-
Patient was apparently alright 3 yrs back then he developed b/l involuntary movements which are asymmetrical(more on right side) and of lesser amplitude and intensity and frequency.
15 days back he developed fever which is of high grade, intermittent in nature and not associated with chills and rigors. He was treated by the local doctor and the fever subsided in 3 days.
H/o dry cough since 10 days which is more at night on lying down.
H/o generalized weakness and decreased appetite since 10 days.
H/o SOB since 10 days.( class 2)
H/o burning sensation in the chest during night which is relieved on taking food since 10 days.
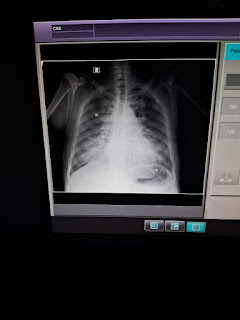
He went to private hospital yesterday afternoon where he was diagnosed to have pneumonia.
Past history-
He is not a k/c/o diabetes,hypertension, tuberculosis, asthma, epilepsy, leprosy, CAD, CVA
Personal history-
Diet -vegetarian
Appetite -decreased since 15 days
Sleep -decreased
B&B movements-regular
Addictions - started consuming alcohol 2 years back(after demise of his wife) and then stopped consuming since 1 year(due to the fear of alcohol affecting his health).
Family history-
No significant family history
GENERAL EXAMINATION :- patient is conscious,coherent and cooperative,well oriented to time place and person.
He is moderately built and nourished.
Pallor - absent

Icterus absent


Cyanosis - absent
Edema of feet - absent
Lymphadenopathy - absent
Clubbing - absent
VITALS:
Temperature: 100 F
BP: 140/80mmhg
PR: 112 bpm
RR : 18CPM
SYSTEMIC EXAMINATION:
CVS - S1, S2 heard , no murmurs
Apex beat localised at 5th ICS
RESPIRATORY SYSTEM-
Position of trachea is central
Shape of chest - cylindrical
BAE present
Breath sounds - Crepts heards at rt infra clavicular, mammary and infra mammary regions and lt mid axillary and infra scapular regions
ABDOMINAL SYSTEM- soft , non tender and mild hepatosplenomegaly


CNS -
Oriented to time, place and person
Able to recall events but there is delay in response
Speech is normal
No cranial nerve deficits
No loss of power
Tone - more increased on right upper limb
??Cog wheel rigidity
Hyper reflexia of biceps, triceps, supinator
2+ for knee reflex
Absent b/l ankle reflex
B/L plantar withdrawal +
Palmomental reflex +
Tremors in both upper limbs &/ hands which is coarse and static


PROVISIONAL DIAGNOSIS -
BICYTOPENIA UNDER EVALUATION
WITH
COMMUNITY ACQUIRED PNEUMONIA WITH (BILATERAL LOWER LOBE CONSOLIDATION) PARKINSON'S(?)WITH
MODERATE SPLEENOMEGALY
TREATMENT -
Inj AUGMENTIN 1.2g/IV/BD
TAB AZITHROMICIN 500 mg/PO/OD
INJ OPTINEURON 1 amp 100 ml /NS
Vital monitoring
Temperature monitoring


Comments
Post a Comment