THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 55 year old male patient
came to casuality with alleged history of seizure activity on 28/2/22 for which he was admitted in a hospital where he was resuscitated and intubated after having cardiac arrest on day 2 (4 am) of his stay at the hospital.
HISTORY OF PRESENTING ILLNESS :
Patient was apparently asymptomatic 6 years then he suffered with sudden onset seizure activity which lasted for 8- 10 minutes on 28/2/22.
He had h/o involuntary movements of upper limb and lower limb with uprolling of eyes along with aura ,involuntary micturition and defecation, tongue bite, post ictal confusion.
He was rushed to a nearby hospital and was treated conservatively .During the stay in the hospital patient had cardiac arrest on day 2 of admission at 4 a.m. was intubated and put on mechanical ventilator and referred to us in view of of their affordability issues.
H/o seizures- 1 st episode 6 yeras back
2 episode 1year back
3 episode on 28/2/22
History of fever since 3 days.
PAST HISTORY:
k/c/o seizures since 6 years.
History of trauma to head 10 years back (fall from bike ) ,no chief complaints of LOC, headache, seizures giddiness.
H/o seizure attack 6 years back for which he was treated with levipril.
1 year back he had another seizure activity since then he was advised to take regular medication ( levipril) to avoid future seizure activity but the patient didn't take regular medication.
Not a known case of DM and HTN.
PERSONAL HISTORY:
Diet - mixed( consumption of pork)
Alcoholic since 15 years , tobacco smoking since 30 years
GENERAL EXAMINATION:
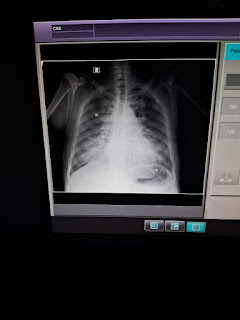
O/E : patient is on mechanical ventilator
FiO2 - 40%
PEEP- 5
VT - 420
GCS: E1 VT M2
Pallor - absent
Icterus absent
Cyanosis - absent
Edema of feet - present
Lymphadenopathy - absent
Clubbing - absent
VITALS:
Temperature: 100 F
BP: 140/80mmhg
PR: 112 bpm
RR : 18CPM
SYSTEMIC EXAMINATION:
CNS:
Pupils - B/L NSRL
Reflexes:
Biceps 2+ 2+
Triceps 2+ 2+
Supinator 2+ 2+
Knee 3+ 3+
Ankle - -
Plantar mute mute
CARDIOVASCULAR SYSTEM :
S1 and S2 heard, no murmurs heard
RESPIRATORY SYSTEM : BAE present,normal vesiculat sounds heard
P/A : soft
INVESTIGATIONS 5/3/22
BGT: B POSITIVE





6/3/22
SPOT URINE PROTEIN: 7
SPOT URINE CREATNINE: 74
RATIO: 0.09



PROVISIONAL DIAGNOSIS:
SEIZURE UNDER EVALUATION (? ALCOHOL WITHDRAWAL SEIZURE) ? HYPOXIC ENCEPHALOPATHY POST CPR STATUS DAY 5
TREATMENT:
HEAD AND ELEVATION UP TO 30%
INJ. MEROPENEM 1 G IV BD
INJ. LEVIPIL 500 MG IV BD
INJ MIDAZOLAM 10 MG IN 50 ML NS @ 30 ML/ hr INJ. MANNITOL 100 ML IV BD
INJ. PANTOP 40 MG IV OD
INJ. NEOMOL 100 ML IF TEMPERATURE > 101 F INJ THIAMINE 2 AMP IN ONE DNS IV BD

Comments
Post a Comment