THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Chief complaints:
Fever and generalized weakness since 16days.
Involuntary movements since 6days.
Pain abdomen and altered sensorium since 4days.
History of presenting illness:
Patient was apparently asymptomatic 16days back then she developed fever with chills and rigor,intermittent in nature and associated with generalized weakness without evening raise of temperature for which she went to local hospital and she treated with some injection.one day later she again developed fever for which she is admitted to local government hospital and got treated.
Since 6days she has a complaints of involuntary movements of upper limbs and jaw.
Since 4days she has a complaint of pain abdomen in epigastric region which is sudden in onset,non progressive,non radiating and associated with one episode of vomiting-which was non bilious and non projectile.
Since 3days she had a complaint of altered sensorium.
Past history:
N/K/C/O of DM,HTN,Asthma,TB,Epilepsy,CAD.
Personal history:
Diet : Mixed
Appetite : Decreased
Sleep : Disturbed
Bowel and Bladder moments :Regular
Addictions:chronic alcoholic since 30yrs, Betelnut chewing since 30yrs
Family history:
Not significant.
General physical examination:
Patient is conscious ,coherent and cooperative and well oriented to time, place and person.
moderately built and nourished.







Pallor-absent
Icterus-absent
Cyanosis-absent
Clubbing-absent
Lymphadenopathy-absent
Edema-absent
Vitals:
Temperature - 99.5*c
PR :- 75bpm
RR :-22cpm
BP :- 110/80mm Hg
SPO2 :- 98%
GRBS :-106mg/dl
Systemic examination:
CVS -S1 S2 heard no murmurs
RS-BAE+
CNS - NFND
P/A-soft, tenderness present over epigastric region.
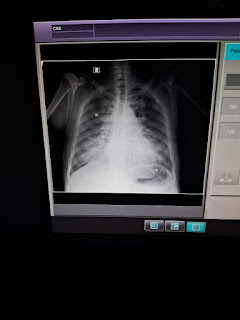
Investigations:







Provisional diagnosis:
Viral pyrexia.
Acallculous cholecystitis.
Alcohol dependence syndrome.
Treatment:
IV fluids-NS,RL,DNS
IV monncef 1mg/iv/BD
Inj Rantac 50mg/iv/OD
Inj PMC 2mg/iv/sos if temp is >102*F
Inj Zofer 4mg/iv/sos
Inj Thiamine 200mg in 100ml NS/if/BD
Tab Prednisolone 10mg/po/OD
Tab Olanzepine(mouth dissolving)2.5mg x 2days


Comments
Post a Comment