A 52 year old male with sob
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 55 year old male patient came to the op with the cheif complaints of sob since 20 days.
HOPI-patient was apparently asymptomatic 20 days back then he developed sob,which was of class 4 (sob even on minimum physical activity and also on rest)(according to nyha).
Since 3-4years patient complains of sob with severe physical activity(class 3) which progressed to current state.
H/o facial puffiness and b/l pedal edema (upto the knee) since 20 days days(facial puffiness resolved currently)
H/o orthopnea since 20 days back.
H/o lower back pain since 4-5years(for that he took nsaids for pain relief 1 tab for 2 days for 3 -4 years)
No h/o palpitations,chest pain, cough,burning micturition, decreased urine output, fever ,cold.
PAST HISTORY- H/O b/l inguinal hernia surgery 8 years back(8 years back on right side and 4 years later on left side)
Not a/k/o D.M,htn,tb,asthma,epilepsy,
seizures,cad.
H/o allery to fish food
No known drug allergies


PERSONAL HISTORY-
diet -mixed
Appetite -normal
Sleep-adequate
Bowel and bladder movements-regular
Addictions- daily drinks 90 ml of whiskey and goes home, and also keeps pan?? Under his lower lip.
DAILY ROUTINE-he wakes up everyday around 8 and goes to the market(vegaetable seller) and wil have breakfast at 10 and then he comes home at 1 to have lunch takes a rest of 1-2 hr and goes back to shop stay there till 8 and drinks 90 ml of alchol comes back home have dinner and sleeps.
FAMILY HISTORY- his mother and elder brother died with complaints of severe sob.
Treatment history-nil
GENERAL EXAMINATION- Patient was conscious,coherant,cooperative,well oriented to time place and person
Pallor- present
Edema-present
Clubbing-present




No icterus,cyanosis,lymphadenopathy
Vitals - temp-afebrile
PR- 68 bpm
RR-20cpm
BP-140/90mmhg
Raised jvp
SYSTEMIC EXAMINATION-
CVS-
INSPECTION:-chest normal in shape,no visible pulsation,no scars, no dilated veins,no percordial bulge seen


PALPATION:- all inspectory findings are confirmed.
Apical impulse felt at-?5 ICS SPACE at lateral to mcl.
No thrills and no heave present.
AUSCULTATION- auscultation done in all 4 areas ,s1 and s2 heard no murmurs heard.
RESPIRATORY SYSYTEM-
Inspection-trachea appears central,chest wall normal,no scars,no sinuses and no dilated veins present
Palpation:- trachea central ,symmetrical expansion of chest seen
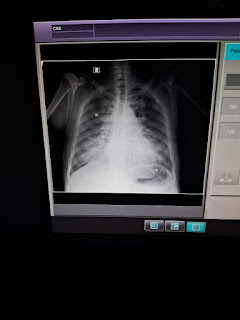
Tactile vocal fremitus -decreased on right mammary and axillary area
Percussion- dullness felt at axillary area on right side
Auscultation-normal vesicular breath sounds heard and diminished sounds at rt mammary and axillary areas,
Cns-no focal neurological deficit
P/a-soft non tender no organo megaly
PROVISIONAL DIAGNOSIS- heart failure with reduced ejection fraction, with pleural effusion with ckd under evaluation.
Investigations-





Treatment-
1.inj lasix 40 mg iv bd
2.fluid restriction <1lt/day and slat restriction <2gm/day.
3.tab.ecosprin po
4. Tab MET-XL 12.5 mg po
5. Inj. Thiamine 200mg direct iv bd
6. Pantop 40 mg po bd
7. Bp charting every 4 th hrly and grbs 12 th hrly

Comments
Post a Comment