THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 58 year old came with chief complaints of
Bilateral pedal edema and sob since 4 days and low grade fever since 2 days.
HOPI-
Patient was apparently asymptomatic 3 years ago then he noticed poor wound healing for which he consulted a local doctor and was diagnosed with diabetes mellitus and was on a OHA. since then.
6 months ago he had a history of giddiness for which he consulted a doctor and was diagnosed with hypertension and using the antihypertensives.
5 months ago he developed bilateral pitting type of pedal edema .
Then on 13/2/2022 He had a H/O s o b grade 4
H/O bilateral pedal edema which is pitting type up to ankles, which is associated with periorbital edema ,
On 13/2/22
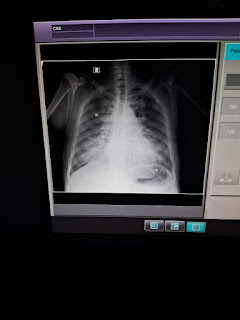
he had H/o decreased appetite, Vomitings( non bilious, non projectile , food as content ) for which he was taken to a hospital in Miryalaguda and was diagnosed as CKD (serum creatinine 9.1 mg/dl) with anaemia (HB 5.8 , normocytic hypochromic) with pulmonary edema with uremic gastritis
Patient then came to the hospital on 19/2/ 2022 . Here patient was managed symptomatically and five sessions of dialysis were done with 2 units of PRBC transfusion and got discharged on 24/2/2022
Now on 8/3/ 22 he came with the complaints of bilateral pedal edema ,sob, facial puffiness, Since 4 days
fever and cough Since 2 days
PEDAL EDEMA is of pitting type, Up to the knees.
SOB - grade 4
H/O FEVER which is low grade , not associated with chills and Rigors
DRY COUGH Insidious in onset, Gradually progressive , No positional and diurnal variation
PAST HISTORY:
PAST HISTORY :
k/c/o Diabetes mellitus type 2 since 3 years and on OH
K/C/O of HTN since 6 months & on regular medication
N/k/c/o BA, TB, THYROID DISORDERS, CVA, EPILEPSY.
left eye - cataract surgery 1 year back.
PERSONAL HISTORY :
DIET : mixed
Appetite : decreased
sleep : adequate
bowel and bladder habits : normal
Addictions : consumes alcohol - 180 ml twice weekly ( since 20 years)
Chews Gutka (since 20 years)
EXAMINATION : Pt is drowsy and arousable
VITALS :
TEMP : 99.2 f
HR : 88 bpm
BP : 130/80 mm hg
RR : 26 cpm
SPO2 : 98 % @ RA
GRBS: 208 mg/dl
Pallor +

B/l pitting edema upto knees.

No icterus, clubbing, lymphadenopathy.
CVS : s1, s2 + . No murmurs
RS : bae + NVBS +
P/A : soft,non tender.
CNS:
Tone Right Left
Elbow Hypertonic Hypertonic
Shoulder Hypertonic Hypertonic
Hips Hypertonic Hypertonic
Knee Hypertonic Hypertonic
Kernig sign Positive
Brudzinski sign Positive
Reflexes Right Left
Biceps 2+ 2+
Triceps 2+ 2+
Supinator 2+ 2+
Knee. - -
Ankle. - -
Babinski No response No response
Lateral rectus palsy + ( false localizing sign )
Investigations:-
RFT
urea -160
Creat- 5.0
UA -2.2
P -5.5
Na -146
k -5.4
Cl -98
Hemogram
HB -9.2
TLC -19,200
PLT- 1.78
MCV -86.3
ABG ON ROOM AIR
pH -3.36
Pco2 -34.9
Hco3 -20.3
Pao2- 95.5
Spo2 -96.3




PROVISIONAL DIAGNOSIS--
CKD with DM and HTN ,meningitis??
Treatment:-
1.fluid restrictions <1.5L/day.
2.salt restrictions <2g/day
3.TAB.LASIX 40mg BD
4.TAB.ECOSPORIN -AV OD
5.TAB.MET-XL 12.5mg OD
6.TAB.NODOSIS 500MG BD
7.TAB.SHELCAL 500MG OD
8.TAB. BIO-D3 0.25MG OD
9.TAB.OROFER-XT OD
10.inj. HAI sc Acc. To Grbs Tid
11.inj ERYTHROPOIETIN 4000U SC x ONCE WEEKLY
INJ. Meropenem 500 mg IV BD
Inj. THIAMINE 1 AMP in 100 ml NS IV BD
INJ. TRAMADOL 1 AMP IN 100 ML NS IV BD
INJ. NEOMOL IV SOS

Comments
Post a Comment